The US government has yet to confirm whether individuals exposed to Ebola will be permitted re-entry under standard protocols for repatriation and medical surveillance.
The escalating Ebola crisis in the Democratic Republic of Congo threatens to surpass previous records, yet Trump's team has failed to outline a coherent strategy for protecting US citizens exposed to the virus so far.
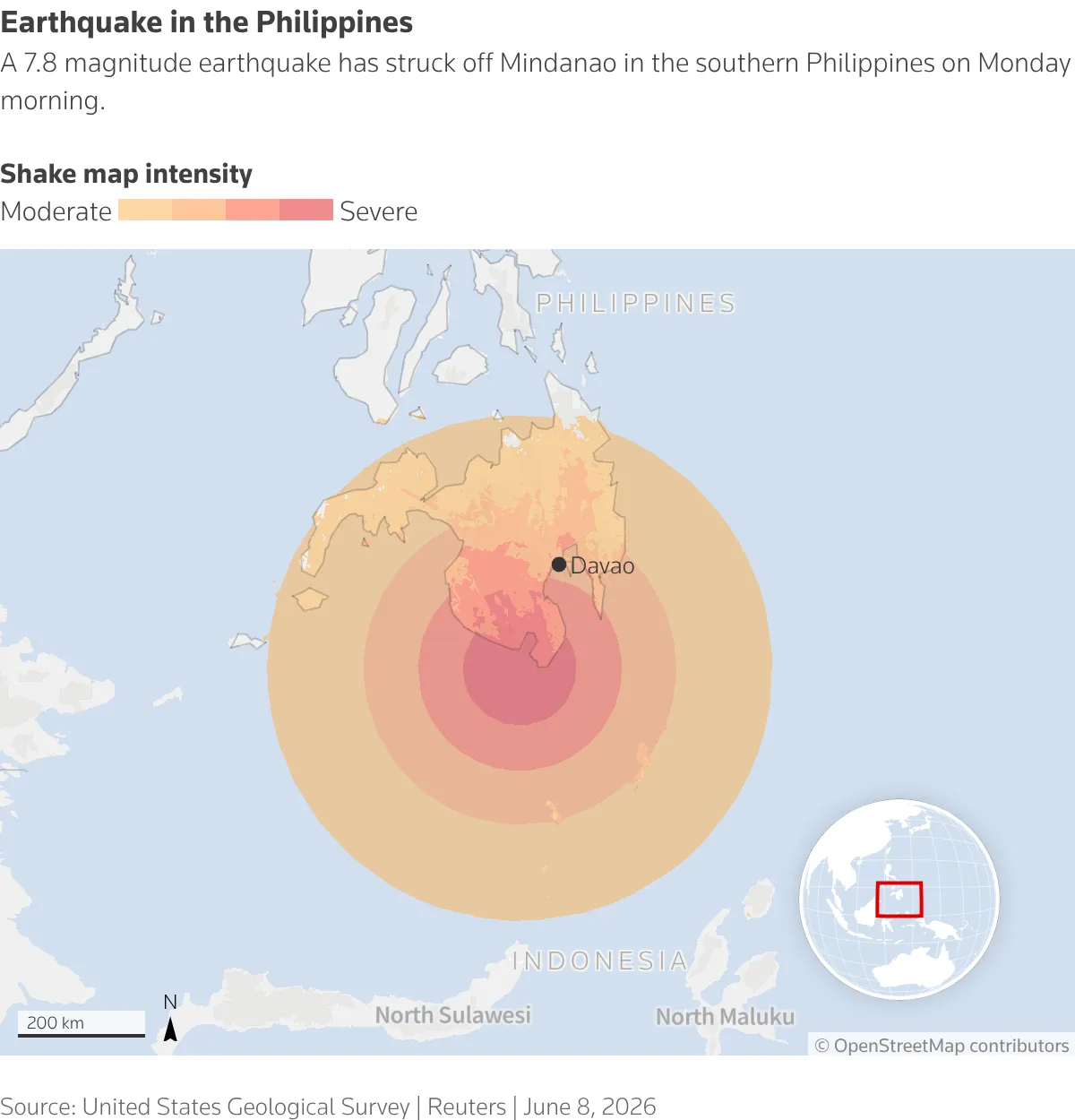
Related ↗A powerful earthquake measuring 7.8 magnitude hits the south of Philippines.Americans, including federal officials, aid workers, and journalists, will soon be present in areas of Congo where Ebola is widespread. According to former administration officials, a well-established protocol exists for individuals exposed to or infected with the virus: they are repatriated to one of 13 specially designed US facilities.
Quarantining Americans abroad is not within the US government's jurisdiction, rendering it powerless to stop their return.
Read next ↗New Obesity Treatment from Boehringer-Zealand Reduces Visceral Liver Fat Effectively.Last week, a stark warning was issued by Secretary of State Marco Rubio: no Ebola cases would be allowed into the US under his administration's watch.
American patients affected by Ebola have been transported to medical facilities abroad: one physician was sent to a German hospital, while six individuals with potential viral exposure are being monitored in Germany and the Czech Republic. No further American cases of high-risk exposure have come to light, according to public health observers following the situation closely.
The administration's proposal to construct a 50-bed quarantine facility in Kenya has hit a roadblock. A Kenyan court's decision on Tuesday has stalled the project, pushing its completion back by at least three weeks. The contingency plan for American citizens requiring assistance remains ambiguous.
Optimism surrounds the prospects of overcoming objections to the Kenya plan, according to a State Department official speaking on Tuesday. However the department has yet to address repeated inquiries regarding U.S. citizens who opt out of travel to Kenya or prefer treatment within the United States, leaving their entry status unclear.
The department clarified that each situation will be evaluated individually.
The public's right to know is being severely compromised during an extremely perilous period for American citizens, according to Lawrence O. Gostin, director of the World Health Organization Collaborating Center on National and Global Health Law.
Ebola crisis expert Mr. Gostin expresses frustration with unclear US efforts, describing them as opaque, confusing, and contradictory in their approach so far.

Confirmed Ebola cases in the Democratic Republic of Congo and Uganda total 359, with 61 fatalities, including a single American victim. Officials anticipate an increase in reported cases as they investigate further and identify additional individuals who may be infected. The outbreak's origins date back several months prior to its detection.
The Ebola virus transmits through direct contact with contaminated bodily fluids. Its rapid progression can cause severe damage to vital organs, ultimately resulting in a swift and tragic demise. Individuals exposed to an infected person, even if asymptomatic, are generally cautioned to closely monitor their health for any signs of the disease.
A Kenyan medical unit was established to monitor Americans exposed to Ebola and provide basic treatment if symptoms arose, all within a 21-day quarantine period. Despite receiving equipment from the US, its capabilities would likely fall short of American facilities' standards. In Liberia during the 2014 outbreak, a comparable medical unit achieved a survival rate of 56 percent, significantly lower than the 81 percent seen in US treatment centers.
The deployment of Public Health Service officers raises concerns about their safety, according to Stephanie Psaki, former coordinator for global health security under the Biden administration, whose position is currently vacant. Deploying personnel without a commitment to repatriate them if they fall ill is morally questionable.
During her time in office from 2021 to 2025, Dawn O'Connell oversaw the procurement of critical equipment, specifically two mobile biocontainment units, designed to ensure extremely safe transportation between airports and nearby hospitals.
The protocols are established to facilitate swift action in response to emergencies.
Lawmakers were informed by Senator Rubio on Tuesday that the administration is weighing several candidates for a key position overseeing the national Ebola response efforts.
President Trump's stance on Ebola has been ambiguous since last week, mirroring his earlier Twitter post from 2014 where he stated unequivocally that the US wouldn't permit EBOLA-infected individuals' return. Those who travel abroad for humanitarian efforts are indeed commendable but must face repercussions.
Immigrants and lawful permanent residents with recent travel history to Congo, Uganda, or South Sudan within the past 21 days are being barred from entry under a public health law invoked by the administration.
A State Department representative, Tommy Pigott, hinted on Tuesday that American travelers in Kenya's Ebola unit can opt out of quarantine if asymptomatic, but those refusing will still face US and international health regulations.
Evacuation procedures for individuals with Ebola symptoms remain shrouded in uncertainty. The State Department has indicated that officials can facilitate transport to predetermined safe areas, though specific destinations have not been disclosed.
Dr. Nahid Bhadelia, Director of Boston University's Center on Emerging Infectious Diseases and experienced Ebola responder, warns that without a clear plan, individuals may conceal their exposure to the virus.
Deploying personnel face a pressing concern: the uncertainty surrounding their safety in Kenya is a significant factor. Those considering volunteering to aid in the outbreak are likely weighing the risks, and unclear consequences may deter some from participating altogether.
Concerns about worker safety are mounting. Established in 2014, the Monrovia Medical Unit in Liberia was a critical initiative by U.S. officials to aid foreign healthcare workers infected with Ebola. Out of 18 confirmed patients treated at this facility, a mere 10 managed to recover.
Dr. Karen Wong, a seasoned Public Health Service officer, reflected on the team's initial deployment to the unit. "Lacking essential gear and trained staff," she noted, "we were ill-equipped to perform complex procedures like intubation."
In stark contrast to previous outbreaks, a significant majority of American evacuees from West Africa in 2014 fared well in US hospitals, with only a small minority succumbing to the disease. Alarmingly, nearly one-quarter of these patients required life-supporting ventilation, and three-quarters needed supplemental oxygen therapy.
In Kenya, a well-equipped medical facility might still struggle with essential resources, including oxygen and basic necessities like intravenous fluids. The availability of vital equipment, such as ventilators, is also uncertain. According to the Department of Health and Human Services, no confirmation was given on whether necessary supplies would be provided.

The Public Health Service officers deployed to Kenya may lack sufficient training to combat Ebola effectively. A comparison between the current three-day training and the more extensive program in 2014 reveals significant disparities, as revealed by a source privy to both initiatives who chose to remain anonymous to avoid repercussions from the Trump administration.
Healthcare professionals in US hospitals often struggle to respond effectively to Ebola due to inadequate training. In Kenya's sweltering environment, medical staff face the daunting task of caring for patients while clad in cumbersome protective suits with limited resources at their disposal.
Dr. Fiona Havers, a seasoned infectious disease specialist and ex-Public Health Service officer, expressed deep unease about providing care to Ebola patients after just three days of training. Her concerns stem from her own experience in Liberia with the Centers for Disease Control and Prevention during the 2014 outbreak, where she supported efforts but didn't treat patients directly.
Nurse epidemiologist Kaci Hickox faced forced isolation in a temporary enclosure near Newark Liberty International Airport upon her 2014 return from Sierra Leone, despite displaying no Ebola symptoms. Her subsequent lawsuit against Maine ultimately resulted in a successful claim for overreach by the state authorities.
Critics argue that this proposal portrays the United States as vulnerable to internal health threats, undermining its ability to protect its citizens effectively.